 对照组,差异具有统计学意义(t=-22.020、-18.393、-7.205,P<0.01);两组患者在复发率及3年存活率上差异无统计学意义(χ2=0.338、0.361,P>0.05);Log-rank 单因素分析显示,肿瘤直径≥5 cm及T 3 期患者的预后较差,为3年RFS及OS的危险因素(χ2=8.183、21.548、8.427、12.410,P<0.01);进一步行Cox 多因素分析,肿瘤直径≥5 cm为术后患者3年RFS的危险因素(RR=3.658,95%CI: 1.875~7.137,P<0.01),T 3 期和肿瘤直径≥5 cm 为影响患者3年OS的危险因素(P<0.01)。 结论 经尿道膀胱肿瘤电切术的手术风险较小,联合辅助静脉、膀胱灌注化疗能够到良好的治疗效果,肿瘤直径≥5 cm、T3期是影响膀胱癌患者预后的重要危险因素。
对照组,差异具有统计学意义(t=-22.020、-18.393、-7.205,P<0.01);两组患者在复发率及3年存活率上差异无统计学意义(χ2=0.338、0.361,P>0.05);Log-rank 单因素分析显示,肿瘤直径≥5 cm及T 3 期患者的预后较差,为3年RFS及OS的危险因素(χ2=8.183、21.548、8.427、12.410,P<0.01);进一步行Cox 多因素分析,肿瘤直径≥5 cm为术后患者3年RFS的危险因素(RR=3.658,95%CI: 1.875~7.137,P<0.01),T 3 期和肿瘤直径≥5 cm 为影响患者3年OS的危险因素(P<0.01)。 结论 经尿道膀胱肿瘤电切术的手术风险较小,联合辅助静脉、膀胱灌注化疗能够到良好的治疗效果,肿瘤直径≥5 cm、T3期是影响膀胱癌患者预后的重要危险因素。
[关键词] 根治性膀胱癌切除术;经尿道电切术; 膀胱肿瘤;预后
[中图分类号] R737 [文献标识码] A [文章编号] 1674-0742(2016)02(b)-0021-03
[Abstract] Objective To compare the efficacy between radical cystectomy and transurethral electroresection in the treatment of muscle-invasive bladder cancer, and analyze the risk factors affecting the prognosis of the patients. Methods 69 cases with muscle-invasive bladder cancer diagnosed and treated in Department of Urologic Surgery of our hospital from January 2005 to October 2012 were selected and divided into the electroresection group(33 cases) and the radical group(36 cases). Patients in the electroresection group were treated by transurethral electroresection of bladder tumor and postoperative intravenous and bladder perfusion chemotherapy, and those in the radical group were treated by radical cystectomy with postoperative intravenous chemotherapy. A 3-year follow-up was given to the patients. The duration of procedure, intraoperative blood loss, cumulative hospitalization time, 3-year recurrence-free survival (RFS), and 3-year overall survival (OS) and so on were compared between the two groups. Potential risk factors were analyzed by univariate Log-rank and multivariate Cox regression. Results Compared with the radical group, the electroresection group had much shorter duration of procedure, much less intraoperative blood loss and obviously shorter length of stay(t=-22.020, -18.393, -7.205, P<0.01). The difference in the recurrence rate and 3-year survival rate between the two groups was not statistically significant (χ2=0.338, 0.361, P>0.05). Log-rank single factor analysis showed that, the prognosis of patients with the diameter of tumor ≥ 5 cm and T3 stage was poor; diameter of tumor ≥ 5 cm and T3 stage in patients were the risk factors of 3-year RFS and 3-year OS (χ2=8.183, 21.548, 8.427, 12.410, P<0.01). Cox multivariate analysis showed that, the diameter of tumor ≥ 5 cm was the risk factor of 3-year RFS (RR=3.658, 95% CI: 1.875~7.137, P<0.01); T3 stage and tumor diameter ≥ 5 cm were the risk factors related to 3-year OS (P<0.01). Conclusion There is low risk of operation in transurethral electroresection of bladder tumor. Transurethral electroresection of bladder tumor combined with intravenous and bladder perfusion chemotherapy can achieve good therapeutic effect. The tumor diameter ≥5 cm and T3 stage are the important risk factors affecting the prognosis in patients with bladder cancer.
[Key words] Radical cystectomy; Transurethral electroresection; Bladder tumor; Prognosis
膀胱肿瘤是泌尿系肿瘤中最常见的肿瘤,占所有恶性肿瘤的20%左右。其中 90%以上为移行上皮癌[1],多发生在三角区、两侧壁及颈部。其中肌层浸润性膀胱癌多已发生远处转移,复发率高,5 年生存率约25%[2-3]。该次研究通过回顾性分析2005年1月—2012年10月于该院泌尿外科诊治的69例肌层浸润性膀胱癌患者的临床资料,探讨经尿道电切术和根治性膀胱切除术治疗的疗效及预后影响因素,现报道如下。
1 资料与方法
1.1 一般资料
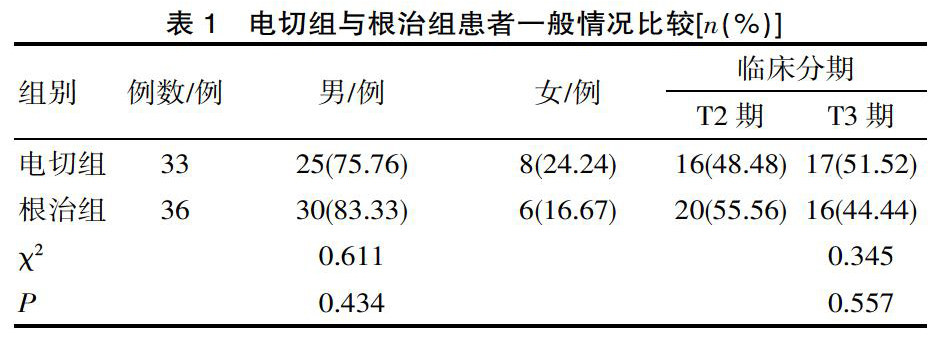
整群选取2005年1月—2012年10月于该院泌尿外科诊治的肌层浸润性膀胱癌患者69例,其中33例患者行尿道电切治疗(电切组),36例行根治性膀胱切除术(根治组),患者肿瘤临床分期为T2、T3期,盆腔淋巴结未见转移。电切组平均年龄(62.34±10.17)岁,根治组平均年龄(64.25±11.26)岁,2组患者性别、肿瘤分期等一般情况,差异无统计学意义(t=0.794,χ2=0.261、0.345,P>0.05)。见表1。
1.2 方法
1.2.1 电切组 经尿道电切镜直视下行手术操作,切除肿瘤至膀胱壁外脂肪层,范围至肿瘤外正常膀胱黏膜组织1.0 ~2.0 cm,生理盐水对膀胱内血块及组织进行冲洗,术后放置三腔气囊留置尿管(F20~F22,国产或进口)反复低压冲洗,视引流尿液的颜色、性状等于3~7 d拔出留置尿管。辅助性化疗在术后1周进行, GC(吉西他滨+顺铂)方案静脉给药,丝裂霉素定期膀胱内灌注。
1.2.2 根治组 气管插管下全身麻醉,患者呈头低脚高仰卧位。于下腹部正中切口,长约 15 cm,经腹或腹膜外膀胱全切除以及盆腔淋巴结扩大清扫,行输尿管皮肤造瘘术、回肠膀胱术或原位新膀胱术以完成尿流改道。术后1周行静脉途径的GC方案。
1.3 疗效观察
比较2组患者的手术时间、术中出血量、累积住院时间;分析影响患者预后的危险因素,其中包括手术方式、年龄、病理分级、肿瘤分期、部位、个数等。定期随访,术后每3个月1次,24个月后每6个月1次,复查内容包括血常规、生化、膀胱镜、胸片、B 超、CT/MRI以及肝肾功能状况,记录肿瘤复发转移、3年无复发生存期(RFS)及3 年总生存率(OS)等。
1.4 统计方法
采用SPSS 17.0软件行数据分析,计量资料以(x±s)表示,组间比较行t检验或非参数Mann-Whitney U检验,单因素分析采用log-rank检验,多因素分析采用COX风险回归模型,计数资料用百分比(%)表示,行χ2检验,P <0.05为差异有统计学意义。
2 结果
2.1 2组患者围手术期情况比较
2组患者手术进展顺利,围手术期无死亡病例。电切组未见穿孔、闭孔反射等并发症,根治组仅1例发生感染,经抗生素治疗后好转。与根治组相比,电切组在手术时间、失血量以及住院时间上明显减少,差异具有统计学意义(t=-22.020、-18.393、-7.205,P<0.01),见表2。
2.2 2组患者术后随访比较
该研究共计随访61例(88.41%),随访时间为38~75个月。电切组失访4例,肿瘤复发13例,原位、异位复发分别6例、7例,其中2例随访中复发3次,复发肿瘤升级,均再次行尿道肿瘤切除术;根治组失访4例,肿瘤复发12例,其中6例患者尿道复发,5例发生淋巴结转移,1例肝转移。2组患者在复发率及3年存活率上差异无统计学意义(χ2=0.338、0.361,P>0.05),见表3。
2.3 2组患者的预后影响因素分析
Log-rank 单因素分析显示,肿瘤直径≥5 cm及T3 期患者的预后较差,为3年RFS及OS的危险因素(χ2=8.183、21.548、8.427、12.410,P<0.01);进一步行Cox 多因素分析,肿瘤直径≥5 cm为术后患者3年RFS的危险因素(RR=3.658,95%CI: 1.875~7.137,P<0.01),T 3 期和肿瘤直径≥5 cm 为影响患者3年OS的危险因素(P<0.01),见表4、5。
3 讨论
膀胱肿瘤为泌尿系肿瘤中最常见的恶性肿瘤,具有较高的发病率和病死率。其中非肌层浸润性膀胱癌约占初发膀胱肿瘤的70%,包括膀胱癌Ta期、T1期及Tis期,进一步可进展为肌层浸润性膀胱癌[4]。根治性膀胱切除术是临床上治疗肌层浸润性膀胱癌的主要选择方式,对原发肿瘤的局部控制效果良好,但同时存在手术复杂、术中失血量多、手术时间长及术后并发症发生率较高等问题[5-6]。而临床研究表明,对于早期诊断的浅肌层浸润、局限性及分化良好的肌层浸润性膀胱癌患者,行尿道膀胱肿瘤电切术联合术后化疗对组织创伤小、机体应激反应轻,可达到良好的治疗效果[7-8]。该次研究结果显示,相较于传统根治性膀胱切除术,经尿道膀胱肿瘤电切术能够明显减少患者手术时间、失血量及累积住院时间,表明后者在围手术期的治疗上效果更好。
该次研究中,通过对肌层浸润性膀胱癌患者术后3年随访资料进行分析,经尿道膀胱肿瘤电切术联合化疗的患者3 年RFS及3年OS均为51.72%,与Hansel DE等[9]和HBZ等[10]研究基本一致。另外,该次研究中2种手术方式的3年RFS及3年OS差异无统计学意义,表明经尿道膀胱肿瘤电切术在肌层浸润性膀胱癌方面存在可行性,但仍需进一步临床研究。
临床研究显示,对膀胱癌患者行尿道膀胱肿瘤电切术时易发生微小肿瘤的漏切,且肿瘤直径>5cm时前列腺癌的风险增加[11]。临床上膀胱T2期肿瘤侵犯肌层(T2a期达浅肌层,T2b期达深肌层),而T3期已侵及膀胱周围组织,易通过组织内丰富的血管、淋巴发生复发和转移。该次研究结果显示,肿瘤直径≥5 cm是导致患者术后肿瘤复发的危险因素,而肿瘤直径≥5 cm、 T 3 期是影响患者3年OS的危险因素。
综上所言,临床上对治疗肌层浸润性膀胱癌的治疗多采用根治性膀胱切除术,而经尿道膀胱肿瘤电切术的手术风险较小,联合辅助静脉、膀胱灌注化疗能够起到良好的治疗效果,且多因素分析显示肿瘤直径≥5 cm、T3期是影响膀胱癌患者预后的重要危险因素。
[参考文献]
[1] Babjuk M, Burger M, Zigeuner R,et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2013[J]. Eur Urol, 2013, 64(4):639-653.
[2] FA Y, JR S, W. K. Contemporary management of muscle-invasive bladder cancer[J]. Expert Rev Anticancer Ther, 2012 ,12(7):941-950.
[3] MJ R, JC B, PE. C. Management of superficial and muscle-invasive urothelial cancers of the bladder[J]. Curr Opin Oncol, 2013, 25(3):281-288.
[4] Cheung G, Sahai A, Billia M, et al. Recent advances in the diagnosis and treatment of bladder cancer[J].BMC Med, 2013, 11(3):42.
[5] 艾星,贾卓敏,孙玉成,等.腹腔镜下根治性膀胱切除术-回肠膀胱术的技术与经验[J].中华泌尿外科杂志,2013,34(8):603-607.
[6] ML K, R E, JE. B. Robotic versus open radical cystectomy: identification of patients who benefit from the robotic approach[J]. J Endourol, 2013, 27(1):40-44.
[7] van Dijk PR,Ploeg M,Aben KK,et al. Downstaging of TURBT-Based Muscle-Invasive Bladder Cancer by Radical Cystectomy Predicts Better Survival[J].ISRN Urol, 2011, 2011: 458930.
[8] 陈伟.经尿道钬激光膀胱肿瘤切除术与经尿道膀胱肿瘤电切术治疗表浅层膀胱癌的疗效和安全性:对比研究[J].中国全科医学,2014,17(2):223-225.
[9] Hansel DE,Amin MB, Comperat E,et al. A contemporary update on pathology standards for bladder cancer: transurethral resection and radical cystectomy specimens[J]. Eur Urol, 2013, 63(2):321-332.
[10] HB Z, SG P, CJ S,et al. Trends in the Utilization of Neoadjuvant Chemotherapy in Muscle-invasive Bladder Cancer: Results From the National Cancer Database[J]. Urology, 2014, 83(1):75-80.
[11] Abdelsalam YM, Mokhtar AA, Kurkar AA,et al. Defining patient selection for prostate-sparing cystectomy in squamous cell carcinoma of the urinary bladder associated with bilharziasis: an overview of 236 patients[J].Urology, 2011, 78(6):1351-1354.
(收稿日期:2015-11-17)